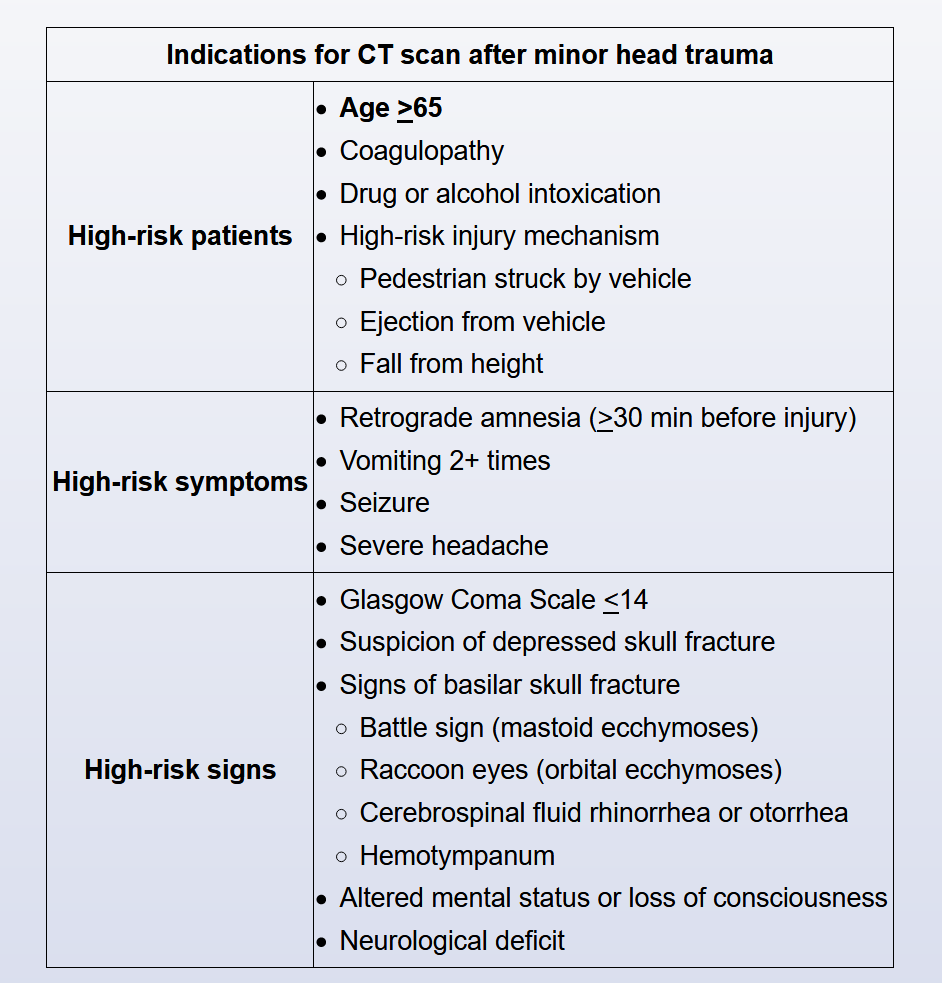
indication for CT scan after minor head trauma
- related: Neurology
This patient has an acute head injury. He did not lose consciousness and has no additional neurological symptoms (eg, vomiting, diplopia) or signs (eg, cranial nerve deficits, altered sensorium). However, elderly patients with seemingly minor trauma may have more extensive injury than is initially apparent; therefore, they warrant more thorough evaluation than younger patients with similar injuries. This patient should be transferred to an acute care emergency department for a CT scan of the head.
Patients age >65 are frequently under-triaged and are at increased risk for occult complications following seemingly minor trauma (eg, head injury, blunt chest injury). These patients may not develop tachycardia or other autonomic signs as readily as younger patients; due to preexisting hypertension they can often have a significant drop in blood pressure and still appear normotensive. Comorbid conditions and medications can add to the risk.
Hospital observation (typically for at least 24 hours) is recommended for patients at risk for complications (eg, decreased level of consciousness, seizure, bleeding disorder or anticoagulant therapy, significant abnormalities discovered on imaging) after imaging is performed.